The birth of a baby with gastroschisis often sends parents into a whirlwind of emotions. Picture this: a couple, anxiously awaiting the arrival of their first child, is shocked to learn, during a routine ultrasound, that their baby has a rare and life-threatening condition where the intestines are outside the body. The initial fear and confusion are overwhelming, but early intervention and surgical repair often lead to surprisingly positive outcomes.
This article doesn’t just cover the basics; it digs into what happens after the diagnosis, offering parents and healthcare professionals actionable insights on managing gastroschisis and its complications.
What is Gastroschisis? The Surprising Truth About This Birth Defect
Gastroschisis is more common than most people think, affecting approximately 1 in every 2,000 births. However, there’s a crucial misunderstanding when it comes to how it’s perceived: many lump it together with other abdominal wall defects like omphalocele, assuming they share the same treatment protocols. The major difference is that in gastroschisis, the baby’s organs—especially the intestines are exposed to amniotic fluid without any protective covering. This can lead to irritation, swelling, and further damage to the organs, making immediate surgical intervention critical.
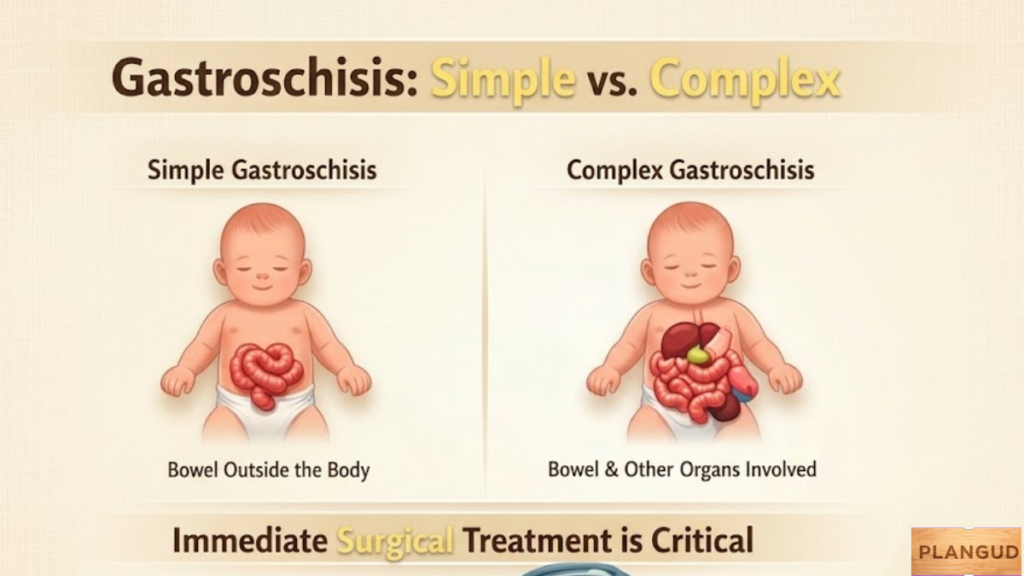
What often gets overlooked is that the severity of gastroschisis can vary. Simple cases, where only the intestines are exposed, are generally easier to manage, while complex gastroschisis, involving multiple organs or intestinal necrosis, requires a more delicate approach. This difference in severity plays a huge role in determining the approach for surgical repair and long-term care.
Diagnosing Gastroschisis: How Early Detection Can Save Lives
The earlierthe gastroschisis is diagnosed, the better the outcome. In many cases, ultrasound detects the condition during the 18-20 week prenatal checkup. The early diagnosis enables doctors to plan for immediate surgical intervention after birth. But here’s the catch: many parents still struggle with the emotional toll of seeing their baby’s organs exposed, even when an early diagnosis is made. This is where the emotional support aspect comes in.
In practice, while the diagnosis can be emotionally overwhelming, the reassurance that surgical repair is a standard procedure helps alleviate fears. Early intervention significantly reduces the risk of long-term gastrointestinal complications, giving the baby a fighting chance.
What Happens After Birth for a Baby With Gastroschisis?
When a baby with gastroschisis is born, the focus shifts to immediate surgery. Typically, the baby will be placed in the NICU, and the medical team will assess the severity of the condition. Primary repair is the most common approach, where the intestines are immediately placed back into the abdomen, and the abdominal wall is repaired. However, in more complex cases, a staged repair is necessary, where the baby’s organs are placed in a silo and gradually moved back inside the body over several days.
The real challenge occurs post-surgery, when feeding difficulties and delayed bowel function often arise. Babies may require TPN (total parenteral nutrition) until they can tolerate breast milk or formula. In the first few weeks, parents may find it difficult to witness their baby’s slow recovery. This is where many get it wrong—while surgical repair is necessary, post-surgery recovery often takes longer than expected.
For instance, one real-world case involved a baby who had to stay in the NICU for over three months. Despite the initial success of surgery, the gastrointestinal complications persisted, requiring multiple follow-up surgeries.
Gastroschisis vs. Omphalocele: What’s the Key Difference?
When parents first hear the term gastroschisis, they may confuse it with omphalocele. While both involve abdominal wall defects and the externalization of organs, the key difference lies in how the organs are exposed. In an omphalocele, the organs are protected by a membrane, whereas in a gastroschisis, there is no protective covering. This means the organs are at a much higher risk of damage, particularly from amniotic fluid, which can lead to intestinal swelling or short bowel syndrome.
In practice, this distinction is essential because gastroschisis requires more urgent care immediately after birth. With omphalocele, the surgery can sometimes be delayed, depending on the severity and the protective covering. This is where many miss the mark. Treatmentprotocols for gastroschisis are more aggressive because of the immediate risk to the baby’s organs, making early diagnosis and intervention crucial.
Is It Possible to Have a Vaginal Delivery with Gastroschisis?
The question of vaginal delivery vs. C-section often arises for parents expecting a baby with gastroschisis. While C-sections are commonly recommended due to the risk of compression on the exposed organs, vaginal delivery is still an option in some cases, especially if the gastroschisis is mild.
But here’s where it gets tricky: In practice, C-section delivery is often preferred to avoid putting pressure on the baby’s exposed intestines. That said, some mothers may opt for a vaginal delivery, and the medical team will monitor the baby closely. It’s important to note that delivery method decisions should be made based on the baby’s condition and the risks involved, not a one-size-fits-all approach.
Surgical Options for Gastroschisis: Primary vs. Staged Repair
There are two main approaches to surgical repair: primary repair and staged repair. Primary repair is typically performed when the baby’s organs are in good condition and can be immediately returned to the abdominal cavity. In contrast, staged repair is necessary for more complex cases, where the intestines are swollen or multiple organs are involved.
The key takeaway here is that many people assume gastroschisis is treated the same way in all cases. However, the severity of the condition directly influences the choice between primary and staged repairs. The real complication lies in the fact that staged repair requires a silo, and this often involves a longer recovery time, with the baby needing intensive monitoring and feeding support.
You may also like: Runlia
Common Mistakes Parents Make After Gastroschisis Surgery and How to Avoid Them
A common mistake parents make post-surgery is expecting immediate recovery. Gastroschisis recovery takes time, and the baby may face issues like intestinal motility problems or feeding difficulties that extend the stay in the NICU. Parents need to stay informed and understand that long-term care may involve ongoing monitoring of the baby’s digestive system.
Another misstep is neglecting emotional support. Parents often focus solely on the physical recovery of the baby and overlook the emotional strain they might be under. This can lead to burnout. Parents need proper guidance and support to cope with the stress of extended hospital stays and the fear of complications.
Conclusion
If you’re a parent of a baby diagnosed with gastroschisis, or a healthcare professional involved in neonatal care, this information is critical. Understanding the different surgical repair options, the need for emotional support, and the realities of post-surgery recovery is essential for managing the condition successfully.
However, if you’re seeking a quick fix or an overly simplistic approach to gastroschisis, this may not be the article for you. The road to recovery is complex, and it requires patience, emotional resilience, and a team-oriented approach to care.
FAQs
Can gastroschisis be detected too early? Should I be worried if it’s found at 12 weeks?
While early detection of gastroschisis is crucial, finding it too early can sometimes lead to misinterpretation of the severity. Some cases may appear more complicated on early scans and may not show the actual extent of the condition at birth. An ultrasound at 12 weeks is generally not as definitive as one done at 18-20 weeks, as the baby’s organs may not have fully developed at that stage. In practice, you might be advised to undergo more frequent monitoring to ensure an accurate diagnosis closer to 20 weeks.
Is it possible to have a baby with gastroschisis and avoid all long-term complications?
While most babies with gastroschisis recover well with early intervention, the possibility of long-term complications like short bowel syndrome or intestinal failure remains, especially in more severe cases. Many babies face ongoing digestive issues like slow motility or feeding difficulties, even after surgery. Realistically, a baby with complicated gastroschisis may need lifelong follow-up care, including potential surgeries, to manage these challenges.
Should I avoid vaginal delivery if my baby has gastroschisis?
Vaginal delivery can be an option, but it should be avoided in cases of severe gastroschisis where multiple organs are exposed or the intestines are swollen. Pressure during vaginal delivery may cause further damage to the exposed organs, which is why a C-section is typically recommended for complex cases. In some rare cases, vaginal delivery can work, but it requires careful consideration and a well-prepared medical team.
What happens when the surgery for gastroschisis fails?
Surgical failure in gastroschisis is rare but possible, particularly if intestinal necrosis or other complications like infection arise. In some edge cases, damage to the intestines from prolonged exposure to amniotic fluid might not be repairable, leading to the need for a bowel transplant or long-term intestinal rehabilitation. The failure rate tends to be higher in complex cases, where the organs are extensively damaged or where the baby’s health is not stable enough for immediate repair.
Are there any hidden risks associated with gastroschisis surgery?
One of the hidden risks of gastroschisis surgery is intestinal blockage after the procedure. The intestines may heal in a way that causes narrowing or strictures, which can lead to feeding difficulties or even intestinal obstruction down the line. These issues may not be immediately apparent post-surgery and can sometimes lead to the need for additional surgeries. In many cases, follow-up care is required to monitor the healing process closely, as some complications develop weeks or months after the initial surgery.
Share this content: